Hebrews 9:27 (KJB) And as it is appointed unto men once to die, but after this the judgment: / What will be your eternal destination ~ Heaven? or Hell?
Luke 9:23 Media
Let Down Your Nets
There is no exclusion put upon any tribe or clan, no classes are laid under ban, no individuals are exempted. Therefore, Church of Christ, by the love you bear to your crucified Master, by His wounds and death for you, and by His living love to you, seek out the lost and gather together the outcasts. You fishers of men, launch out into the deep and let down your nets for a draught. You sowers of holy seed, go abroad, and sow the untrodden wastes. You consecrated builders, break away from old foundations, and lay fresh groundwork for a larger temple for your God and King. Surely the Spirit of love in a church will suggest this. ~ C. H. Spurgeon
16 For I am not ashamed of the gospel of Christ: for it is the power of God unto salvation to every one that believeth; to the Jew first, and also to the Greek. 17 For therein is the righteousness of God revealed from faith to faith: as it is written, The just shall live by faith. ~ Romans 1:16, 17
28 Whom we preach, warning every man, and teaching every man in all wisdom; that we may present every man perfect in Christ Jesus: ~ Colossians 1:28
16 And without controversy great is the mystery of godliness: God was manifest in the flesh, justified in the Spirit, seen of angels, preached unto the Gentiles, believed on in the world, received up into glory. ~ 1 Timothy 3:16
6 Jesus saith unto him, I am the way, the truth, and the life: no man cometh unto the Father, but by me. ~ John 14:6
21 For he hath made him to be sin for us, who knew no sin; that we might be made the righteousness of God in him. ~ 2 Corinthians 5:21
25 Jesus said unto her, I am the resurrection, and the life: he that believeth in me, though he were dead, yet shall he live: 26 And whosoever liveth and believeth in me shall never die. Believest thou this? ~ John 11:25,26
16 For God so loved the world, that he gave his only begotten Son, that whosoever believeth in him should not perish, but have everlasting life. 17 For God sent not his Son into the world to condemn the world; but that the world through him might be saved. 18 He that believeth on him is not condemned: but he that believeth not is condemned already, because he hath not believed in the name of the only begotten Son of God. ~ John 3:16-18
24 Wherefore the law was our schoolmaster to bring us unto Christ, that we might be justified by faith. ~ Galatians 3:24
23 For the wages of sin is death; but the gift of God is eternal life through Jesus Christ our Lord. ~ Romans 6:23
8 For by grace are ye saved through faith; and that not of yourselves: it is the gift of God: 9 Not of works, lest any man should boast. 10 For we are his workmanship, created in Christ Jesus unto good works, which God hath before ordained that we should walk in them. ~ Ephesians 2:8-10
3 Jesus answered and said unto him, Verily, verily, I say unto thee, Except a man be born again, he cannot see the kingdom of God. 7 Marvel not that I said unto thee, Ye must be born again.~ John 3:3,7
3 For this is good and acceptable in the sight of God our Saviour; 4 Who will have all men to be saved, and to come unto the knowledge of the truth. 5 For there is one God, and one mediator between God and men, the man Christ Jesus; ~ 1 Timothy 2:3-5
13 The God of Abraham, and of Isaac, and of Jacob, the God of our fathers, hath glorified his Son Jesus; whom ye delivered up, and denied him in the presence of Pilate, when he was determined to let him go. 14 But ye denied the Holy One and the Just, and desired a murderer to be granted unto you; 15 And killed the Prince of life, whom God hath raised from the dead; whereof we are witnesses. ~ Acts 3:13-15
19 Repent ye therefore, and be converted, that your sins may be blotted out, when the times of refreshing shall come from the presence of the Lord; 20 And he shall send Jesus Christ, which before was preached unto you: 21 Whom the heaven must receive until the times of restitution of all things, which God hath spoken by the mouth of all his holy prophets since the world began. ~ Acts 3:19-21
36 He that believeth on the Son hath everlasting life: and he that believeth not the Son shall not see life; but the wrath of God abideth on him. ~ John 3:36
11 And this is the record, that God hath given to us eternal life, and this life is in his Son. 12 He that hath the Son hath life; and he that hath not the Son of God hath not life. ~ 1 John 5:11,12
21 He that hath my commandments, and keepeth them, he it is that loveth me: and he that loveth me shall be loved of my Father, and I will love him, and will manifest myself to him. ~ John 14:21
7 For there are three that bear record in heaven, the Father, the Word, and the Holy Ghost: and these three are one. ~ 1 John 5:7
IF YOUR BOSS THREATENS YOU WITH FIRING IF NOT VACCINATED DON’T REFUSE:
The secret is NOT to refuse the jab and do not sign anything!
From a lawyer:
If you are being forced to Vax in order to keep your job, here’s a great way to handle it. (Conditional acceptance)
The secret is NOT to refuse it.
“I write with regard to the matter of potential covid vaccine and my desire to be fully informed and appraised of ALL facts before going ahead. I’d be most grateful if you could please provide the following information, in accordance with statutory legal requirements.”:
1. Can you please advise the approved legal status of any vaccine and if it is experimental?
2. Can you please provide details and assurances that the vaccine has been fully, independently and rigorously tested against control groups and the subsequent outcomes of those tests?
3. Can you please advise the entire list of contents of the vaccine I am to receive and if any are toxic to the body?
4. Can you please fully advise of all the adverse reactions associated with this vaccine since it’s introduction?
5. Can you please confirm that the vaccine you are advocating is NOT experimental mRNA gene altering therapy?
6. Can you please confirm that I will not be under any duress from yourselves as my employers, in compliance with the Nuremberg Code?
7. Can you please advise me of the likely risk of fatality, should I be unfortunate to contract Covid 19 and the likelihood of recovery?
8. Can you please advise me if I were to experience any adverse reactions is the manufacturer of the vaccine liable? If the manufacturer isn’t liable will the company I’m currently employed with with be responsible & liable as it is their request that I have the vaccine in order to carry on my employment?
Once I have received the above information in full and I am satisfied that there is NO threat to my health, I will be happy to accept your offer to receive the treatment, but with certain conditions – namely that:
1. You confirm in writing that I will suffer no harm.
2. Following acceptance of this, the offer must be signed by a fully qualified doctor who will take full legal and financial responsibility for any injuries occurring to myself, and/or from any interactions by authorized personnel regarding these procedures.
3. In the event that I should have to decline the offer of vaccination, please confirm that it will not compromise my position and that I will not suffer prejudice and discrimination as a result?
I would also advise that my inalienable rights are reserved.
The point is that if they CANNOT provide that information you’ve NOT refused.
Rumble — The legal issues may feel overwhelming. Julia Haller, Attorney at Law breaks it down for the rest of us. For More resources and information, visit https://defendingtherepublic.org/covid/
We get medical and scientific information which is precise as the above video reveals, and then you get absolute rubbish spewed from the South African Acting Minister of Health Mr Joe Phaala to promote the COVID-19 jab amongst 12 to 17 year olds. In the following Eyewitness News (EWN) video, Mr Phaala goes on record, reading from his script, and says, quote:
The vaccine Ministerial Advisory Committee advised that for now we should only give one dose of Pfizer while assessing information, eh we suggest in few cases all over the world there have been some short lived cases of trysiant myocarditis after the second dose. Now eh this rare finding of this adverse effect it is (stumble and mumble) it is a slight inflammation on the heart muscle which has been noticed in a few cases and the vaccine MAC has advised that while this has been monitored all over the world, at this stage there has been no indication that eh, eh, eh the first dose has any serious side effects, so, for now it would be just one dose while the studies are continued which we believe that will still offer significant protection and once more information come then we can space the second dose for for the young people. But we can assure parents and the young people that even where this has been noticed it has had no permanent risk, so we just taking precaution in this case.
His statements are contradictory and untrue in that there are serious risks with myocarditis which leads to cardiac issues and deaths, many deaths that have been reported around the world. The following reports need to be studied, especially by the South African National Department of Health, SAMA, and SAHPRA –
When it comes to the Acting Director-General of the Health Department Mr Nicholas Crisp pushing the issue surrounding 12 to 17 year olds giving their own consent in the above EWN video, it is not rocket science that many 12 to 17 year olds would not have the mental capacity to make an informed decision, consent or assent to taking the experimental COVID-19 jabs, as they are still under EUA and not bona fide vaccines, after reading up on the adverse side effects, injuries and death that these “vaccinations” can cause. This is total madness and is child abuse as even clinical trials have shown that 86% of children received adverse effects from these toxic jabs - 86% of Children suffered an Adverse Reaction to the Pfizer Covid Vaccine in Clinical Trial – Rights and Freedoms (wordpress.com)
13 He that answereth a matter before he heareth it, it is folly and shame unto him. ~ Proverbs 18:13 KJV
The original LifeSiteNews article that is shared hereunder can be viewed at this Link. Kindly note that since this article has been published the link to the VigiAccess website appears to have been censored by being taken down by the technocratic fact-checking thought police. This is not new as all truth is being censored! To obtain information concerning post vaccine adverse injuries and deaths do visit the American website VAERS (Vaccine Adverse Event Reporting System) to search reported data. For South African users kindly visit the website SAVAERS. Kindly note that these VAERS websites mentioned here do not reflect all vaccine injuries and deaths as many people do not come forward and report the same, personally or in the event of death by their next-of-kin.
After all information that has been researched concerning the so-called “vaccines” that are unsafe and only being used by EUA – that is Emergency Use Authorisation – the SAMA (South African Medical Association) has the audacity to come out and want to discipline medical professionals who have another view on the forced vaccine narrative. This smacks of tyrannical dictatorship. Where has one’s democratic freedom of expression and choice gone if one cannot exercise one’s rights under the Bill of Rights? The article in question can be viewed here: ‘Doctors sharing anti-vaccine views MUST be disciplined’ – SAMA (msn.com) We implore all South Africans to record all adverse effects, injuries and deaths so the true facts can be made known. We also implore South African doctors and nurses to make known the true facts behind the “secrecy” of the real facts that are not shared with the general public. It is also known that many governmental frontline medical employees had to sign NDAs (Non Disclosure Agreements), especially those in the “established field hospitals”, like the one at the Pietermaritzburg Royal Show Grounds, when the COVID Pandemic reached our country. Why the secrecy?? This is urgent, as the the South African government take their cue also from the WHO.
Now for the article hereunder . . .
____________________________
NEWS
WHO database reports over 2 million potential COVID jab injuries in 2021, vast majority in women
2,199,476 adverse effects following vaccination against COVID-19 have been reported in 2021 as of today, with 866,558 (39 percent) of the injuries being reported in 18–44-year-olds, and 1,517,989 (69 percent) of all injuries occurring in women.
World Health Organization symbol at WHO headquarters
(LifeSiteNews) — The World Health Organization’s publicly accessible database recording reported potential side effects of medicinal products shows over 2 million cases of possible COVID vaccine injuries in 2021 alone, with 69 percent of the cases occurring in female patients.
VigiAccess was founded in 2015 by the World Health Organization (WHO) to allow the public access to VigiBase, the WHO’s database.
According to VigiAccess, 2,199,476 adverse effects following vaccination against COVID-19 have been reported in 2021 as of today, with 866,558 (39 percent) of the injuries being reported in 18–44-year-olds, and 1,517,989 (69 percent) of all injuries occurring in women.
The database’s Adverse Drug Reactions (ADRS) tab allows the public to see the nature of the injuries that have been reported, including blood and lymphatic system disorders, cardiac disorders, musculoskeletal and connective tissue disorders, reproductive system and breast disorders, respiratory, thoracic and mediastinal disorders, and many others.
Looking specifically at some of the disorders and ailments listed under the broad headings, the shocking number of injuries include incidences of vaginal hemorrhaging, myocarditis, brain neoplasms (tumors), spontaneous abortion, fetal death, stillbirth, pulmonary embolism, renal failure, fetal growth restriction, deep vein thrombosis, as well as the onset of COVID-19, influenza, pneumonia, and over 100 other conditions.
There is not currently a function that allows the public to determine which COVID-19 vaccines are correlated with which injuries, but instead all the COVID vaccines and all the injuries are grouped into the same file.
The shocking revelation that 1,517,989 (69 percent) of the cases were reported in the female population could substantiate claims made by various doctors, scientists, and healthcare workers who have fielded concerns regarding the impact the jabs have on women, especially their reproductive organs and their fertility.
In March, Idaho doctor Ryan Cole, a board-certified pathologist and owner and operator of a diagnostics lab, told the public with support of the state government that he is seeing a “20 times increase” of endometrial cancers since the vaccine rollout.
Cole also reported a substantial increase in the rate of melanomas in patients since the vaccine rollout, particularly “thick” melanomas in “younger” patients. According to Cole, it is extremely uncommon to find such progressive melanomas in the younger age ranges.
In Germany, researchers carried out a study that involved the injection of lipid “nanocarriers,” including some with an ingredient common to both Pfizer’s and Moderna’s mRNA COVID vaccines: polyethylene glycol.
The researchers found “high local accumulation of nanoparticles” in “specific locations of the ovaries,” which led the specialized pharmaceutical technology and biopharmaceutics scientists to warn that this may pose a “toxicity issue in humans” and that more research needs to be conducted.
Dr. Michael Yeadon, a former vice president at Pfizer, also fielded his concerns about the vaccines’ impact on women’s health when he discovered “data showing that 15 pregnant women who were vaccinated [against COVID] developed three-fold higher levels of antibodies against their own placentas” and that this data was “dismissed and hidden by the vaccine industry and public health.”
Further, Dr. Elizabeth Lee Vliet, an independent physician specializing in reproductive hormones, referenced a 2018 study where Chinese researchers found that nanoparticles [like the particles used in the mRNA vaccines] can pass through the blood–testis barrier, placental barrier, and barriers protecting reproductive tissues, and then accumulate in reproductive organs.
According to Vliet, per the Chinese study, the accumulation of nanoparticles damages organs (testis, epididymis, ovary, and uterus) by destroying specific cells, leading to reproductive organ dysfunction that adversely affects sperm and eggs and may disrupt the ovarian cycle.
The WHO is far from the only major player in the medical world to reveal the injurious and even deadly impact the COVID-19 vaccines have had on the public.
The European Union (EU)’s drug database has also reported over 2 million adverse reactions to the jabs, with 1 million being considered serious, and over 21,000 resulting in death.
Additionally, Thomas Renz, an American attorney leading a lawsuit seeking to stop the approved use of the COVID-19 vaccines, revealed that he has the sworn testimony of a person working in healthcare data analytics that vaccine injuries are “under-reported by a conservative factor of at least 5.”
Analyzing the data, Renz and his associates aiding with the case announced that the “most conservative estimate” of deaths caused by the jab in America is 45,000, with additional evidence showing it could be “astronomically higher.”
As stated by Texas cardiologist and leading medical expert Dr. Peter McCullough, “Americans are going to bear the brunt of what invariably is going to be a failed mass vaccination program that will go down as one of the most deadly, one of the most injurious and costly in human history.
13 He that answereth a matter before he heareth it, it is folly and shame unto him. ~ Proverbs 18:13 KJV
Do Masks Really Save Lives?
Since the start of the COVID-19 pandemic, health experts have struggled to come together about mask recommendations. Know the two times wearing a mask makes sense and what the latest science says about mask wearing for everyone.
____________________________
Mindless Mask Mandates Likely Do More Harm Than Good
While the media claims mask mandates are based on science and will “save lives,” science is actually ignored wholesale and recommendations are primarily pushed based on emotional justifications and triggers
Recommendations have fluctuated wildly from initially admonishing people to not wear masks, to mandating universal mask wearing by all, including the healthy, to wearing two, three and even four masks, plus goggles and face shields
The logical reason for all this flip-flopping is because actual science is being ignored. From the start, the available research has been rather consistent: Mask wearing does not reduce the prevalence of viral illness and asymptomatic spread is exceedingly rare, if not nonexistent
The largest COVID-19-specific mask trial to date found masks may either reduce your risk of SARS-CoV-2 infection by as much as 46%, or increase it by 23%. Either way, the vast majority — 97.9% of those who didn’t wear masks, and 98.2% of those who did — remained infection free
The U.S. Centers for Disease Control and Prevention rely on an anecdotal story about two hair stylists who interacted with clients while symptomatic. Because everyone wore masks in the salon, and none tested positive after exposure, they claim this is evidence that the masks prevented the spread of infection. Meanwhile, other CDC data reveal 85% of confirmed COVID-19 patients used masks “often” or “always”
This article was previously published February 17, 2021, and has been updated with new information.
In breathless tones, NBC News recently reported1 the existence of a business where mask wearing isn’t enforced. In the Naples, Florida, grocery store, hardly anyone wears a mask. The store’s owner, who the news station claimed “is known for his conservative and often controversial viewpoints,” told a reporter he’s never worn a mask in his life and never will.
The store does have a mask policy posted, but video shows that many customers are fine with not wearing one. There is a mask mandate in Naples, but Florida Gov. Ron DeSantis has issued a ruling that makes enforcement of the rule difficult, NBC said.
The irony of the whole thing is that while the media claims mask mandates are based on science and will “save lives,” this simply isn’t true. Science is actually being ignored wholesale and recommendations are primarily pushed based on emotional justifications and triggers. If science were actually followed, universal mask wearing by healthy people would not — indeed could not — be recommended.
A Timeline of Unscientific Extremes
From the start of the COVID-19 pandemic, health experts have been unable to unify around a cohesive message about face masks. In February 2020, Surgeon General Jerome Adams sent out a tweet urging Americans to stop buying masks, saying they are “NOT effective.”2 (He has since deleted that tweet.) Adams also warned that if worn or handled improperly, face masks can increase your risk of infection.3
Similarly, in March 2020, Dr. Anthony Fauci stated4 that “people should not be walking around with masks” because “it’s not providing the perfect protection that people think that it is.” Logically, only symptomatic individuals and health care workers were urged to wear them.
Fauci even pointed out that mask wearing has “unintended consequences” as “people keep fiddling with their mask and they keep touching their face,” which may actually increase the risk of contracting and/or spreading the virus.
By June 2020, universal mask mandates became the norm and we were told we had to wear them because there may be asymptomatic super-spreaders among us. Interestingly enough, that same month, the World Health Organization admitted that asymptomatic transmission was “very rare.” If that’s true, then why should healthy, asymptomatic people mask up?
By July 2020, Fauci claimed his initial dismissal of face masks had been in error and that he’d downplayed their importance simply to ensure there would be a sufficient supply for health care workers, who need them most.5
Fast-forward a few weeks, and by the end of July 2020, Fauci went to the next extreme, flouting the recommendation to wear goggles and full face shields in addition to a mask, ostensibly because the mucous membranes of your eyes could potentially serve as entryways for viruses as well.6
This despite the fact that a March 31, 2020, report7 in JAMA Ophthalmology found SARS-CoV-2-positive conjunctival specimens (i.e., specimens taken from the eye) in just 5.2% of confirmed COVID-19 patients (two out of 28).
What’s more, contamination of the eyes is likely primarily the result of touching your eyes with contaminated fingers. If you wear goggles or a face shield, you may actually be more prone to touch your eyes to rub away sweat, condensation and/or scratch an itch.
Toward the end of November 2020, the asymptomatic spread narrative was effectively destroyed by the publication of a Chinese study8 involving nearly 9.9 million individuals. It revealed not a single case of COVID-19 could be traced to an asymptomatic individual who had tested positive.
____________________________________
“The logical reason for all this flip-flopping is because actual science is NOT being taken into account. From the start, the available research has been rather consistent: Mask wearing does not reduce the prevalence of viral illness and asymptomatic spread is exceedingly rare, if not nonexistent.”
____________________________________
Around December 2020, recommendations for double-masking emerged,9 and this trend gained momentum through extensive media coverage as we moved into the first weeks of 2021.10 Undeterred by scientific evidence and logic alike, by the end of January 2021, “experts” started promoting the use of three11,12 or even four13 masks, whether you’re symptomatic or not.
These recommendations quickly sparked a mild backlash, with other experts encouraging the return to common sense, as wearing three or more masks may impair airflow, which can worsen any number of health conditions.
True to form, while promoting the concept of double-masking as recently as January 29, 2021,14 by February 1, Fauci conceded “There is no data that indicates double-masking is effective,” but that “There are many people who feel … if you really want to have an extra little bit of protection, ‘maybe I should put two masks on.'”15 In other words, the suggestion is based on emotion, not actual science.
The Singular Truth Behind Mixed Messaging About Masks
The logical reason for all this flip-flopping is because actual science is NOT being taken into account. From the start, the available research has been rather consistent: Mask wearing does not reduce the prevalence of viral illness and asymptomatic spread is exceedingly rare, if not nonexistent.
Both of these scientific consensuses negate the rationale for universal mask wearing by healthy (asymptomatic) people. The only time mask wearing makes sense is in a hospital setting and if you are actually symptomatic and need to be around others, and even then, you need to be aware that it provides only limited protection.
The reason for this is because the virus is aerosolized and spreads through the air. Aerosolized viruses — especially SARS-CoV-2, which is about half the size of influenza viruses — cannot be blocked by a mask, as explained in my interview with Denis Rancourt, who has conducted a thorough review of the published science on masks and viral transmission.
According to Rancourt, “NONE of these well-designed studies that are intended to remove observational bias found a statistically significant advantage of wearing a mask versus not wearing a mask.”
COVID-19 Specific Mask Trial Failed to Prove Benefit
While most mask studies have looked at influenza, the first COVID-19-specific randomized controlled surgical mask trial, published November 18, 2020, confirmed previous findings, showing that:16,17
a. Masks may reduce your risk of SARS-CoV-2 infection by as much as 46%, or it may actually increase your risk by 23%
b. The vast majority — 97.9% of those who didn’t wear masks, and 98.2% of those who did — remained infection free
The study included 3,030 individuals assigned to wear a surgical face mask and 2,994 unmasked controls. Of them, 80.7% completed the study. Based on the adherence scores reported, 46% of participants always wore the mask as recommended, 47% predominantly as recommended and 7% failed to follow recommendations.
Among mask wearers, 1.8% ended up testing positive for SARS-CoV-2, compared to 2.1% among controls. When they removed the people who reported not adhering to the recommendations for use, the results remained the same — 1.8%, which suggests adherence makes no significant difference.
Among those who reported wearing their face mask “exactly as instructed,” 2% tested positive for SARS-CoV-2 compared to 2.1% of the controls. So, essentially, we’re destroying economies and lives around the world to protect a tiny minority from getting a positive PCR test result which means little to nothing.
CDC Relies on Anecdotal Data to Promote Mask Use
If you want additional proof that health authorities are not concerned with following the best available science, look no further than the U.S. Centers for Disease Control and Prevention.18 What do they rely on as the primary piece of “evidence” to back up its mask recommendation?
A wholly anecdotal story about two symptomatic hair stylists who interacted with 139 clients during eight days is all they offer. Sixty-seven of the clients agreed to be interviewed and tested. None tested positive for SARS-CoV-2.
The fact that the stylists and all clients “universally wore masks in the salon” is therefore seen as evidence that the masks prevented the spread of infection. The Danish study reviewed above didn’t even make it onto the CDC’s list of studies.
The CDC’s own data19,20,21 also show 70.6% of COVID-19 patients reported “always” wearing a cloth mask or face covering in the 14 days preceding their illness; 14.4% reported having worn a mask “often.” So, a total of 85% of people who came down with COVID-19 had “often” or “always” worn a mask.
This too contradicts the idea that mask wearing will protect against the infection, and is probably a slightly more reliable indicator of effectiveness than the anecdotal hairdresser story.
Another recent investigation22 revealed the same trend, showing that states with mask mandates had an average of 27 positive SARS-CoV-2 “cases” per 100,000 people, whereas states with no mask mandates had just 17 cases per 100,000.
Masks Don’t Protect Against Smoke
The CDC also contradicts its own conclusions that masks protect against viral spread by specifying that wearing a cloth face mask will NOT protect you against wildfire smoke, because “they do not catch small, harmful particles in smoke that can harm your health.”23 To get any protection from harmful smoke particles, you’d have to use an N95 respirator.
The particulate matter in wildfire smoke can range from 2.5 micrometers in diameter or smaller in smoke and haze, to 10 micrometers in wind-blown dust.24 SARS-CoV-2, meanwhile, has a diameter between 0.06 and 0.14 micrometers, far tinier than the particulate found in smoke.
SARS-CoV-2 is also about half the size of most viruses, which tend to measure between 0.02 microns to 0.3 microns.25 Meanwhile, virus-laden saliva or respiratory droplets expelled when talking or coughing measure between 5 and 10 micrometers.26
N95 masks can filter particles as small as 0.3 microns,27 so they may prevent a majority of respiratory droplets from escaping, but not aerosolized viruses. Influenza viruses and SARS-CoV-2 are small enough to float in the air column, so as long as you can still breathe, they can flow in and out of your respiratory tract.
The following video offers a simple demonstration of how masks “work.” Or rather, don’t, as the vapor flows in and out, all around the mask — even if you’re wearing two of them.
More Science
If you’re still on the fence about whether masks are a necessity that must be forced on everyone, including young children, I urge you to take the time to actually read through some of the studies that have been published. In addition to the research reviewed above, here’s a sampling of what else you’ll find when you start searching for data on face masks as a strategy to prevent viral infection:
Surgical masks and N95 masks perform about the same — A 2009 study28 published in JAMA compared the effectiveness of surgical masks and N95 respirators to prevent seasonal influenza in a hospital setting; 24% of the nurses in the surgical mask group still got the flu, as did 23% of those who wore N95 respirators.
Cloth masks perform far worse than medical masks — A study29 published in 2015 found health care workers who wore cloth masks had the highest rates of influenza-like illness and laboratory-confirmed respiratory virus infections, when compared to those wearing medical masks or controls (who used standard practices that included occasional medical mask wearing).
Compared to controls and the medical mask group, those wearing cloth masks had a 72% higher rate of lab-confirmed viral infections. According to the authors:
“Penetration of cloth masks by particles was almost 97% and medical masks 44%. This study is the first RCT of cloth masks, and the results caution against the use of cloth masks … Moisture retention, reuse of cloth masks and poor filtration may result in increased risk of infection.”
“No evidence” masks prevent transmission of flu in hospital setting — In September 2018, the Ontario Nurses Association (ONA) won its second of two grievances filed against the Toronto Academic Health Science Network’s (TAHSN) “vaccinate or mask” policy. As reported by the ONA:30
“After reviewing extensive expert evidence submitted … Arbitrator William Kaplan, in his September 6 decision,31 found that St. Michael’s VOM policy is ‘illogical and makes no sense’ …
In 2015, Arbitrator James Hayes struck down the same type of policy in an arbitration that included other Ontario hospitals across the province … Hayes found there was ‘scant evidence’ that forcing nurses to use masks reduced the transmission of influenza to patients …
ONA’s well-regarded expert witnesses, including Toronto infection control expert Dr. Michael Gardam, Quebec epidemiologist Dr. Gaston De Serres, and Dr. Lisa Brosseau, an American expert on masks, testified that there was … no evidence that forcing healthy nurses to wear masks during the influenza season did anything to prevent transmission of influenza in hospitals.
They further testified that nurses who have no symptoms are unlikely to be a real source of transmission and that it was not logical to force healthy unvaccinated nurses to mask.”
No significant reduction in flu transmission when used in community setting — A policy review paper32 published in Emerging Infectious Diseases in May 2020, which reviewed “the evidence base on the effectiveness of nonpharmaceutical personal protective measures … in non-healthcare settings” concluded, based on 10 randomized controlled trials, that there was “no significant reduction in influenza transmission with the use of face masks …”
Risk reduction may be due to chance — In 2019, a review of interventions for flu epidemics published by the World Health Organization concluded the evidence for face masks was slim, and may be due to chance:33
“Ten relevant RCTs were identified for this review and meta-analysis to quantify the efficacy of community-based use of face masks …
In the pooled analysis, although the point estimates suggested a relative risk reduction in laboratory-confirmed influenza of 22% in the face mask group, and a reduction of 8% in the face mask group regardless of whether or not hand hygiene was also enhanced, the evidence was insufficient to exclude chance as an explanation for the reduced risk of transdamission.”
“No evidence” that universal masking prevents COVID-19 — A 2020 guidance memo by the World Health Organization pointed out that:34
“Meta-analyses in systematic literature reviews have reported that the use of N95 respirators compared with the use of medical masks is not associated with any statistically significant lower risk of the clinical respiratory illness outcomes or laboratory-confirmed influenza or viral infections …
At present, there is no direct evidence (from studies on COVID- 19 and in healthy people in the community) on the effectiveness of universal masking of healthy people in the community to prevent infection with respiratory viruses, including COVID-19.”
Mask or no mask, same difference — A meta-analysis and scientific review35 led by respected researcher Thomas Jefferson, cofounder of the Cochrane Collaboration, posted on the prepublication server medRxiv in April 2020, found that, compared to no mask, mask wearing in the general population or among health care workers did not reduce influenza-like illness cases or influenza.
In one study, which looked at quarantined workers, it actually increased the risk of contracting influenza, but lowered the risk of influenza-like illness. They also found there was no difference between surgical masks and N95 respirators.
Statistics Show Mask Use Has No Impact on Infection Rates
Another way to shed light on whether masks work or not is to compare infection rates (read: positive test rates) before and after the implementation of universal mask mandates. In his article,36 “These 12 Graphs Show Mask Mandates Do Nothing to Stop COVID,” bioengineer Yinon Weiss does just that.
He points out that “No matter how strictly mask laws are enforced nor the level of mask compliance the population follows, cases all fall and rise around the same time.” To see all of the graphs, check out Weiss’ article37 or Twitter thread.38 Here are just a select few to bring home the point:
To Pose a Risk, You Need To Be Symptomatic
Studies have repeatedly shown that masks do not significantly reduce transmission of viruses, so it’s safe to assume that a mask will in fact fail in this regard. That leaves two key factors: There must be a contagious person around, and they must be sufficiently close for transmission to occur.
We now know that asymptomatic individuals — even if they test positive using a PCR test — are highly unlikely to be contagious.39 So, really, a key prevention strategy for COVID-19 seems to be to stay home if you have symptoms. As for masking up when you’re healthy, let alone double, triple or quadruple masking, there’s simply no scientific consensus for that strategy.
13 He that answereth a matter before he heareth it, it is folly and shame unto him. ~ Proverbs 18:13 KJV
Proof It’s Impossible for Vaccines to Create Herd Immunity
This hospital outbreak, where 96% of exposed patients and staff had been fully vaccinated, tells us the COVID shots cannot create herd immunity. In fact, vaccinated people may be more prone to serious and lethal infection.
A recent report details a SARS-CoV-2 Delta outbreak in an Israeli hospital where 238 out of 248 (96%) of the exposed patients and staff had been fully vaccinated with Pfizer’s mRNA vaccine
Of the 238 fully vaccinated individuals, 39 (16%) were infected, as were three of the 10 unvaccinated individuals who got exposed
While all of the sickened staff recovered, five infected patients died and nine turned into severe or critical cases. All of the dead and severe/critical cases were fully vaccinated. Two unvaccinated patients that got infected only had mild illness
This outbreak tells us that the COVID shots cannot create herd immunity. It also suggests vaccinated people may be more prone to serious and lethal infection than the unvaccinated
Of 41,552 hospitalized patients in the U.S., 73% of the unvaccinated, 71% of the partially vaccinated and 72% of the fully vaccinated received a diagnosis of COVID-like illness (CLI) between January 1, 2021, and June 22, 2021
As we enter into the 10th month of COVID injections, what can we tell about their effectiveness? Are they working? According to data from Israel — which is the best in the world at this point, thanks to the Israelis’ dedication to data collection and transparency — it seems the news is anything but good, and that is a profoundly serious understatement.
In an October 3, 2021, substack article,1 Alex Berenson dissects a recent Eurosurveillance report2 about a SARS-CoV-2 Delta outbreak in an Israeli dialysis ward. Eurosurveillance is a journal published by the European Centers for Disease Control.
Hospital Outbreak Reveals the Ineffectiveness of COVID Jabs
An unidentified dialysis patient came in for scheduled treatment with fever and cough. Over the course of several days, his condition continued to deteriorate, but he remained in the dialysis unit at the Meir Medical Center.
COVID measures at the hospital includes routine wearing of full protective equipment by all COVID unit staff, including N-95 mask, face shield, gown, gloves and hair cover. Patients also wear surgical masks when in the same room as another patient.
By the time the sick patient was tested and diagnosed with COVID-19, he had a PCR cycle threshold (CT) of 13.6, which means he had a viral load approximately 1 million times higher than a person with mild infection.
____________________________________
“This communication … challenges the assumption that high universal vaccination rates will lead to herd immunity and prevent COVID-19 outbreaks… In the outbreak described here, 96.2% of the exposed population was vaccinated. ~ Eurosurveillance October 3, 2021”
____________________________________
The infection spread rapidly among patients and staff, spreading from the dialysis ward to the COVID-19 ward and other units. At the time of the outbreak, 238 out of 248 (96%) of the exposed patients and staff had been fully vaccinated with Pfizer’s mRNA vaccine. Of the 238 fully vaccinated individuals, 39 (16%) were infected, as were three of the 10 unvaccinated individuals who got exposed.
Near-Maximum Vaccination Rate Yet No Herd Immunity
While all of the sickened staff recovered, five infected patients died and nine turned into severe or critical cases. All of the dead and severe/critical cases were fully vaccinated. Two unvaccinated patients who were infected only had mild illness. As noted by the authors:3
“The calculated attack rate among all exposed patients and staff was 10.6% (16/151) for staff and 23.7% (23/97) for patients, in a population with 96.2% vaccination rate (238 vaccinated/248 exposed individuals).
Moreover, several transmissions probably occurred between two individuals both wearing surgical masks, and in one instance using full PPE, including N-95 mask, face shield, gown and gloves …
This nosocomial outbreak exemplifies the high transmissibility of the SARS-CoV-2 Delta variant among twice vaccinated and masked individuals. This suggests some waning of immunity, albeit still providing protection for individuals without comorbidities …
This communication … challenges the assumption that high universal vaccination rates will lead to herd immunity and prevent COVID-19 outbreaks…
In the outbreak described here, 96.2% of the exposed population was vaccinated. Infection advanced rapidly (many cases became symptomatic within 2 days of exposure), and viral load was high.
Another accepted view is that, when facing a possible mismatch between the SARS-CoV-2 variant and vaccine or waning immunity, the combination of vaccine and face mask should provide the necessary protection.
Although some transmission between staff members could have occurred without masks, all transmissions between patients and staff occurred between masked and vaccinated individuals, as experienced in an outbreak from Finland.”
This case tells us a couple of important things. First, that even in a population where more than 96% are fully vaccinated, outbreaks will occur. This means the shots are clearly not even remotely creating any kind of herd immunity. Indeed, there have been outbreaks even in populations where the vaccination rate was 100%.4
Secondly, the unvaccinated who got sick had only mild illness, while the fully vaccinated all ended up with severe infection. The unvaccinated recovered without a problem while several of the fully vaccinated patients died.
Thirdly, it tells us masks, face shields and gloves provide little more than a false sense of security. Altogether, this report is evidence that everything we’re currently doing is foolishness.
COVID-Like Illness Among the Vaccinated
In the U.S., the data are far more manipulated, as this next section will reveal. The study5 in question, “Effectiveness of COVID-19 Vaccines in Ambulatory and Inpatient Care Settings,” was published September 8, 2021, in The New England Journal of Medicine.
The researchers identified a total of 103,199 hospitalizations between January 1, 2021, and June 22, 2021. Of those, 41,552 met the study criteria for inclusion (the real number is actually 41,159, as there’s a mathematical error6). Included patients were 50 or older, and had “COVID-like illness” (CLI), defined as COVID symptoms and a positive PCR test.
Excluded hospitalizations that did not meet the study criteria were patients younger than 50, patients without vaccination record, repeat admissions, patients that had no COVID test results, and those who had received their second dose of mRNA injection (or first and only dose required of the Janssen vaccine) within the last 14 days and therefore were not considered fully vaccinated.
The exclusion of people who got the jab within 14 days of their hospitalization is more than regrettable and designed to create real misinformation and fraudulent results skewed in favor of the jab. Researchers have determined that you’re at increased risk of infection during the first 14 days, because you haven’t reached adequate antibody levels yet.
A Swedish study7 posted April 21, 2021, found “The estimated vaccine effectiveness in preventing infection ≥7 days after second dose was 86% but only 42% ≥14 days after a single dose.” While maximum effectiveness isn’t reached until the 14-day mark, why shouldn’t hospitalizations that occur within that two-week window count?
According to The New England Journal of Medicine report, the effectiveness of the mRNA shots against lab-confirmed SARS-CoV-2 infection, 14 or more days after injection, was 89%, on average. Effectiveness among those 85 and older, those with chronic medical conditions, as well as Black and Hispanic adults, ranged from 81% to 95%.
The effectiveness of the Janssen “vaccine” against lab-confirmed infection leading to hospitalization was 68%, and 73% against infection requiring emergency care. That sounds pretty good, but it doesn’t tell the whole story.
Digging Further Into the Data
In a Twitter thread,8 Ben M. double-checked and recalculated the vaccine efficacy, taking into account all CLI admissions, not just those where the patient had been vaccinated at least 14 days prior. When adding those previously excluded patients back in, Ben M. came up with a vaccine effectiveness rate of 13%.
He also discovered that if you look at how many people actually had a CLI clinical diagnosis code among the 41,552 included patients, the rate of diagnosis between the unvaccinated, the partially vaccinated and the fully vaccinated was nearly identical: 73% for the unvaccinated, 71% for the partially vaccinated and 72% for the fully vaccinated.
Here’s where it gets interesting. When you look at the rate of CLI, and add in the rate of positive PCR tests, all of a sudden, differences between the groups become clear. Only 2% of the fully vaccinated had a positive PCR test, compared to 6% of the partially vaccinated and 18% of the unvaccinated.
Ben M. speculates that vaccinated patients may be tested less routinely (12.5% less frequently to be exact), or unvaccinated patients are tested more routinely (11% more frequently than the vaccinated). But there may be another explanation. The U.S. Centers for Disease Control and Prevention actually has two different sets of testing criteria, depending on the patient’s vaccination status.
Fully vaccinated individuals suspected of having contracted COVID-19 are to be tested using a CT of 28 or less, whereas unvaccinated patients are to be tested using a CT of 40.
Anything over 35 CTs has been shown to produce 97% false positives,9 so this biased testing guidance virtually guarantees that vaccinated patients are more likely to test negative, while unvaccinated patients are more likely to get a false positive.
Partially Vaxxed Are the Most Symptomatic for CLI
What’s more, when Ben M. looked at symptoms alone, he found that the partially vaccinated are the most symptomatic for CLI (29.2%), followed by the fully vaccinated (28.1%) and then the unvaccinated (27.4%).
When he then recalculated vaccine effectiveness based on symptomatic CLI alone (i.e., with or without a positive test), it again came out negative: -6% in the partially vaccinated and -3% in the fully vaccinated. As noted by Ben M. “this means that despite COVID-19 vaccination, people appear to get as sick and hospitalized (if not even more!), as before?!”
He provides a whole series of helpful visuals in his Twitter thread, so to get a clearer idea, I recommend reading through it and looking through all the graphs provided.10 In summary, what Ben M. discovered is that:
• The rate of CLI admission, diagnosis and symptoms are nearly identical between the unvaccinated and vaccinated, so there’s no indication that the COVID shot reduces CLI.
• Sample exclusions distort the data, making the COVID shots appear more effective.
• Of the included hospitalizations for CLI, 53% were either partially or fully vaccinated, compared to 47% unvaccinated.
As of June 15, 2021, 48.7% of Americans were fully “vaccinated,”11 so the distribution of unvaccinated and fully vaccinated individuals being admitted to hospital should have been close to 50/50 by June 22, 2021, which was the cutoff date in this study.
The rate of partially vaccinated has trended about 8% to 10% higher, which would put the vaccinated to unvaccinated ratio at around 60/40. If you assume the number of vaccinated people over the age of 50 was the same as the number of unvaccinated, or just slightly higher, the fact that 53% of CLI cases were vaccinated and 47% were unvaccinated, it suggests the rate of CLI is nearly identical regardless of vaccination status.
• To tease out why vaccinated people develop CLI at the same rate as the unvaccinated, we need all-cause hospitalization and death data by vaccination status, but even though the CDC has acknowledged to Ben M. that they have this data, they denied his Freedom of Information Act request to obtain it.
No Correlation Between Vaccination Rates and COVID Cases
In related news, Blaze Media recently reported the findings of Harvard researchers, who found “absolutely no correlation between vax rates and COVID cases globally.”12 The paper’s title tells you pretty much tells the whole story and everything you need to know: “Increases in COVID-19 Are Unrelated to Levels of Vaccination Across 68 Countries and 2,947 Counties in the United States.”13 According to the authors:
“… the narrative related to the ongoing surge of new cases in the United States (US) is argued to be driven by areas with low vaccination rates. A similar narrative also has been observed in countries …
We used COVID-19 data provided by the Our World in Data for cross-country analysis, available as of September 3, 2021 …We included 68 countries that met the following criteria: had second dose vaccine data available; had COVID-19 case data available; had population data available; and the last update of data was within 3 days prior to or on September 3, 2021.
For the 7 days preceding September 3, 2021 we computed the COVID-19 cases per 1 million people for each country as well as the percentage of population that is fully vaccinated … The percentage increase in COVID-19 cases was calculated based on the difference in cases from the last 7 days and the 7 days preceding them …
At the country-level, there appears to be no discernable relationship between percentage of population fully vaccinated and new COVID-19 cases in the last 7 days. In fact, the trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people.
Notably, Israel with over 60% of their population fully vaccinated had the highest COVID-19 cases per 1 million people in the last 7 days. The lack of a meaningful association between percentage population fully vaccinated and new COVID-19 cases is further exemplified, for instance, by comparison of Iceland and Portugal.
Both countries have over 75% of their population fully vaccinated and have more COVID-19 cases per 1 million people than countries such as Vietnam and South Africa that have around 10% of their population fully vaccinated.
Across the U.S. counties too, the median new COVID-19 cases per 100,000 people in the last 7 days is largely similar across the categories of percent population fully vaccinated … There also appears to be no significant signaling of COVID-19 cases decreasing with higher percentages of population fully vaccinated …
The sole reliance on vaccination as a primary strategy to mitigate COVID-19 and its adverse consequences needs to be re-examined … Other pharmacological and non-pharmacological interventions may need to be put in place alongside increasing vaccination rates.
Such course correction, especially with regards to the policy narrative, becomes paramount with emerging scientific evidence on real world effectiveness of the vaccines.
For instance, in a report released from the Ministry of Health in Israel, the effectiveness of 2 doses of the BNT162b2 (Pfizer-BioNTech) vaccine against preventing COVID-19 infection was reported to be 39%, substantially lower than the trial efficacy of 96%.
It is also emerging that immunity derived from the Pfizer-BioNTech vaccine may not be as strong as immunity acquired through recovery from the COVID-19 virus. A substantial decline in immunity from mRNA vaccines 6-months post immunization has also been reported.
Even though vaccinations offers protection to individuals against severe hospitalization and death, the CDC reported an increase from 0.01 to 9% and 0 to 15.1% (between January to May 2021) in the rates of hospitalizations and deaths, respectively, amongst the fully vaccinated.”
13 He that answereth a matter before he heareth it, it is folly and shame unto him. ~ Proverbs 18:13 KJV
Has COVID Pushed the Masses Into a Delusional Cult?
The phrase ‘drink the Kool-Aid’ originates from events in Jonestown in 1978 in which over 900 people died for an extreme cause. And we may have morphed into a similar form of mass delusional psychosis due to the fear of COVID, according to this doctor.
____________________________
The World Is Suffering From Mass Delusional Psychosis
According to psychiatrist and medical legal expert Dr. Mark McDonald, the true public health crisis is not COVID-19 itself; rather, it’s the fear of the infection, which has “morphed and evolved into a form of mass delusional psychosis”
Many enter a state of hysteria when they see an unmasked person, even if they look perfectly healthy and clearly are not suffering from any kind of respiratory issue. This is a highly irrational state that has no basis in reality
Delusion is defined as believing something that doesn’t conform with reality
There are serious concerns about the lasting effects this widespread insanity will have on children as they grow up. One of the worst traumas children suffer as a result of all this fearmongering is the idea that they may kill their parents or grandparents simply by being around them
Treating the children’s trauma in therapy is not going to be enough, as parents and other adults are the ones creating the trauma by their own exaggerated fear response. To heal a generation of traumatized children, we must first address the psychosis of the adult population
This article was previously published February 18, 2021, and has been updated with new information.
A number of mental health experts have expressed concern over the blatant fear and panic mongering during the COVID-19 pandemic, warning about potential — and let’s face it, likely — psychiatric effects. In a December 22, 2020, article1 in Evie Magazine, S.G. Cheah discusses what may in fact be the real problem at hand: mass insanity caused by “delusional fear of COVID-19.”
Cheah refers to lectures and articles by psychiatrist and medical legal expert Dr. Mark McDonald,2 who believes “the true public health crisis lies in the widespread fear which morphed and evolved into a form of mass delusional psychosis.”
“Even when the statistics point to the extremely low fatality rate among children and young adults (measuring 0.002% at age 10 and 0.01% at 25), the young and the healthy are still terrorized by the chokehold of irrational fear when faced with the coronavirus,” Cheah writes.
Infectious Hysteria
Cheah goes on to review a number of irrational behaviors that have become all too commonplace, such as parents being kicked off planes because their young children refuse to wear a mask during the flight, or people having hysterical meltdowns when they see a person not wearing a mask.
The science3 is quite clear about the risk posed by asymptomatic individuals, meaning anyone who feels perfectly healthy yet may have tested positive for SARS-CoV-2 with a PCR test set to an excessively high cycle threshold. They pose an exceptionally low risk to others, if any risk at all. Science is even clearer on healthy individuals who test negative for SARS-CoV-2. You simply cannot spread a virus you do not have.
The bulk of published science4,5,6,7,8,9,10 also shows that masks do not prevent the spread of viral infections, and this is particularly true if you’re wearing cloth masks,11 surgical masks or masks with vents.
Despite all of that, many still enter a state of hysteria when they see an unmasked person, even if they look perfectly healthy and clearly are not suffering from any kind of respiratory issue. This is a highly irrational state that has no basis in reality.
Indeed, according to McDonald, these people are suffering from delusional psychosis,12 and there are a lot of them. He goes so far as to refer to the outside of his home or office as the “outdoor insane asylum,” where he must assume “that any person that I run into is insane” unless they prove otherwise.13 As explained by Cheah:14
“Instead of facing reality, the delusional person would rather live in their world of make-believe. But in order to keep faking reality, they’ll have to make sure that everyone else around them also pretends to live in their imaginary world.
In simpler words, the delusional person rejects reality. And in this rejection of reality, others have to play along with how they view the world, otherwise, their world will not make sense to them. It’s why the delusional person will get angry when they face someone who doesn’t conform to their world view …
It’s one of the reasons why you’re seeing so many people who’d happily approve the silencing of any medical experts whose views contradict the WHO or CDC guidelines. ‘Obey the rules!’ becomes more important than questioning if the rules were legitimate to begin with.”
In his interview with Jesse Lee Peterson (video above), McDonald explains his diagnosis this way:
“There was never a medical crisis. There were always enough resources to deal with the people who were sick … Many resources were in fact turned away … The question then, for me, became, ‘What’s the real crisis? What are people really suffering from?’
It became clear to me, very quickly, within the first two or three weeks in March [2020], that it was fear. Since then … the fear … has morphed and evolved, not just into a ‘I’m worried, I’m scared so I need to stay home,’ but an actual belief that is against reality — because the definition of delusion is something you believe that doesn’t conform with reality.
They believe that they are going to die — no matter what age, no matter what state of health they’re in — if they don’t leave their house with a mask and gloves on every day and run from [other] human beings. That’s delusional psychosis. It’s false, it’s wrong, it’s not backed up by evidence. And many, many Americans are living that and believing that.”
While there’s no data to back this up, McDonald says it appears women tend to be more prone to delusional psychosis than men. Part of it, he suggests, may be because when women get scared, they tend to become more hyperprotective than men under the same circumstances, likely because women — speaking in pure generalizing terms, of course — tend to be more emotionally driven.
Mass Delusional Psychosis Traumatizes Children
McDonald is particularly concerned with the lasting effects this widespread insanity will have on children as they grow up. As a psychiatrist specializing in the treatment of children and adolescents, he should know. Since the lockdowns began in the first quarter of 2020, he’s seen a massive increase in patients, and their mental states are far worse than what he’s used to seeing in these age groups.
One of the worst traumas children suffer as a result of all this fearmongering is the idea that they may kill their parents or grandparents simply by being around them. As noted by Cheah, they’re also being taught to feel guilty about behaviors that would normally be completely, well, normal.
Just one example is hysterical adults calling a toddler who refuses to wear a mask a “brat,” when in fact resisting having a restrictive mask put across your face is perfectly normal at that age.
“It’s not normal for children to grow up thinking that everyone is a danger to everyone else,” Cheah says, and rightly so. It’s not normal at all, and hysterical adults are mindlessly inflicting severe emotional trauma on an entire generation.
As noted by McDonald in his interview with Peterson above, a primary cause of depression, especially among youngsters, is disconnection from others. We need face-to-face contact, we need physical contact as well as emotional intimacy. We need these things to feel safe around others and within our own selves. Digital interactions simply cannot replace these most basic human needs, and are inherently separating rather than connective.
McDonald cites recent CDC statistics showing there’s been a 400% increase in adolescent depression compared to one year ago, and in 25% of cases, they’ve contemplated suicide. These are unheard of statistics, he says. Never before have so many teenagers considered committing suicide.
“This is a mass-casualty event,” McDonald says, and parents — adults — are to blame, because they are the ones scaring them to the point they don’t feel life is worth living anymore.
This is also why just treating the children is not going to be effective enough. We have to address the psychosis of the adult population. “It’s up to us adults to fix this,” McDonald says, “because children are not going to be able to fix this themselves.”
Delusional People Ultimately Require Controlled Environments
We must also address the mass delusion for another reason, and that is because it’s driving us all, sane and insane alike, toward a society devoid of all previous freedoms and civil liberties, and the corrupt individuals in charge will not voluntarily relinquish power once we’ve given it to them.
A totalitarian society, McDonald believes, is the ultimate end of this societal psychosis unless we do something about it and realize that “we’re fine, we’re perfectly safe.” Indeed, we’re in no more danger now than we were pre-COVID. We must not allow our freedoms to be taken from us due to delusional fears. As noted by Cheah in her article:15
“It’s not unthinkable that the final outcome would be total societal control on every aspect of your life. Consider this — the endpoint of a mentally ill person is for them to be put under a controlled environment (institutionalized like an asylum) where all freedoms are restricted. And it’s looking more and more like that’s the endpoint of where this mass psychosis is heading.”
A December 18, 2020, Tweet by political commentator Candace Owens also sums up how irrational fear and panic have figuratively lobotomized a significant portion of the public:
McDonald points out that many of our leaders obviously do not suffer these same delusional fears. They issue stay-at-home orders from their vacation homes in the Caribbean and repeatedly break their own mask and lockdown mandates. They ride their bikes, stroll through the park, have family gatherings and dine out without a care. They know COVID-19 isn’t the deadly plague it’s been made out to be, but they’re playing the game because it benefits them.
The video above features a short lecture McDonald gave during America’s Frontline Doctors’ White Coat Summit 216 in mid-October 2020, titled “The Way Forward: Overcoming Fear.”
In it, he points out that not only has fear morphed into a delusional belief that masks, gloves and physical separation are required to stay alive, but fear has also been turned into a virtue, which is doubly tragic and wrong.
Wearing a mask has become a way to demonstrate that you’re a “good person,” someone who obviously cares about others, whereas not wearing a mask brands you as an inconsiderate lout, if not a prospective mass murderer, simply by breathing.
____________________________________
“Healthy people should never wear masks, social distance or self-isolate. Not only are these strategies unhealthy from a physical standpoint, they also perpetuate the delusional psychosis gripping the nation and therefore must end.”
____________________________________
By encouraging us to remain in fear, to burrow and settle into it and allow it to control and constrain our lives, the fear has become so entrenched that anyone who says we need to be fearless and fight for our freedoms is attacked for being not only stupid but also dangerous. “I would argue that it’s the opposite,” McDonald says.
The problem we now face is that the delusion has taken such hold that even if the mask mandates ended nationwide today, many would refuse to give up their masks, and they would not stop chastising those who don’t wear them, either. What’s more, we now have private companies pushing these freedom-robbing edicts, refusing services to those who don’t wear masks.
Already, certain venues across the U.S.17 and around the world18 won’t allow you in if you don’t have the COVID-19 vaccine, and private corporations are the ones instigating those unconstitutional rules. Even U.S. President Joe Biden is pushing vaccine mandates for admission to entertainment venues.19
If you understand the technocratic agenda, then you know why that is. It’s because many private companies are part of the global technocratic alliance that is trying to eliminate our freedoms in order to enrich themselves.
“We started out with fear and hysteria. We moved to delusional psychosis, and now we have group control,” McDonald says. “Now we don’t have police officers and government coming after us. What we have more of is our fellow citizens now castigating us, legally limiting us from getting into vehicles [such as Uber or plane], going into businesses [and] getting jobs.”
Restoring Sanity as We Move Forward
Essentially, citizens are now acting as a de facto “police force” to suppress other people’s freedom, and this has a terribly harmful effect on society. So, how do we get out of the proverbial insane asylum? How do we restore sanity to our society while still helping those who are at greatest risk for complications and death from COVID-19? McDonald offers the following suggestions in his lecture and the featured interview:
We must firmly reject masks as a virtue signal; the idea is that action taken out of fear — such as donning a mask — is virtuous. Fear is not helpful and never virtuous.
We should protect those at greatest risk — meaning elderly, frail individuals with comorbidities and those who are in poor health.
Healthy people should never wear masks, social distance or self-isolate. Not only are these strategies unhealthy from a physical standpoint, they also perpetuate the delusional psychosis gripping the nation and therefore must end.
We must embrace courage, truth, honesty and freedom, not just in our thoughts and words but also in our actions. As noted by McDonald in the featured interview, people cannot think logically when in a state of delusional psychosis, hence sharing information, facts, data and evidence tends to be ineffective except in cases where the person was acting out of peer pressure rather than a delusional belief.
Typically, the best you can do is stand firm and act in alignment with truth and objective reality, much like you would if you were a first responder faced with an accident victim who is responding hysterically to what you know is only a minor injury.
13 He that answereth a matter before he heareth it, it is folly and shame unto him. ~ Proverbs 18:13 KJV
‘Papers Please’: Vaccine Passports Have Arrived
For a weary public longing to get back to normalcy, vaccine passports represent a tantalizing carrot being dangled ahead for freedom. Don’t be fooled; they are setting the stage for increased surveillance and an erosion of your privacy.
____________________________
‘Papers, Please’: Vaccine Passports Have Officially Arrived
The U.K. government has given sizable grants to a number of private companies developing vaccine passports and digital certificates that show vaccination status
It’s likely only a matter of time before you’ll be asked to prove your vaccination status in order to carry on with your daily life
This blatant move toward an ever-increasing surveillance state is being welcomed by many who have been led to believe they’re necessary to protect public health and safety
In the U.S., universities continue to institute lockdowns for students, going so far as to ban even outdoor exercise
While many countries have suggested that the COVID-19 vaccine will not be mandated, by giving special privileges to the vaccinated, such as the ability to travel, attend social events or even enter a workplace, it essentially amounts to the same thing and insinuates a “cleaner” class of people in those who have been vaccinated
This article was previously published February 24, 2021, and has been updated with new information.
For a weary public longing to get back to normalcy, vaccine passports represent a tantalizing carrot, being dangled as a mechanism for freedom. By showing proof that you’ve received a COVID-19 vaccine, perhaps you can once again board an airplane and travel freely, attend a concert or enjoy a meal in your favorite restaurant, just like you used to.
Except, being required to present your “papers” in order to live your life isn’t actually freedom at all — it’s discrimination, and even a move toward technocratic fascism, one that’s setting the stage for increased surveillance and erosion of your privacy.
Nonetheless, this blatant move toward an ever-increasing surveillance state is being welcomed by many who have been led to believe the passports are necessary to protect public health and safety.
Vaccine Passports Are in Development
It’s likely only a matter of time before you’ll be asked to prove your vaccination status in order to carry on with your daily life. “The government seems to be developing vaccine passports by stealth, making sure the technology is in place for anyone who needs it,” wrote Lara Prendergast, The Spectator’s assistant editor.1
She’s referring to the U.K. government, which has given sizable grants to a number of private companies developing such technology. This includes more than $86,000 to Logifect, to create and launch a vaccine passport app,2 and more than $104,000 to iProov and Mvine, which are developing digital certificates that show vaccination status.
As Prendergast noted, “Your phone would most likely be your vaccination passport. Everyone’s vaccination status is already being logged centrally by the National Immunization Vaccination System using their NHS number. This information could be easily linked with an app.”3
Around the world, vaccine passports are rapidly being rolled out, including in Denmark, which was one of the first to roll them out.4 As of September 2021, dozens of countries around the world have implemented vaccine passports,5 while in the U.S., plans for vaccine IDs are under evaluation.6 International efforts are also underway.
The Commons Project and the World Economic Forum created the Common Trust Network, which developed the CommonPass app that’s intended to act as a health passport.
The app allows users to upload medical data such as a COVID-19 test result or proof of vaccination, which then generates a QR code that you will show to authorities as your health passport.7 The proposed common framework “for safe border reopening” around the world involves the following:8
Every nation must publish their health screening criteria for entry into the country using a standard format on a common framework
Each country must register trusted facilities that conduct COVID-19 lab testing for foreign travel and administer vaccines listed in the CommonPass registry
Each country will accept health screening status from foreign visitors through apps and services built on the CommonPass framework
Patient identification is to be collected at the time of sample collection and/or vaccination using an international standard
The CommonPass framework will be integrated into flight and hotel reservation check-in processes
Eventually, the CommonPass framework will be integrated with already existing personal health apps such as Apple Health and CommonHealth. If you want to travel, your personal health record will be evaluated and compared to a country’s entry requirements, and if you don’t meet them, you’ll be directed to an approved testing and vaccination location.
Majority Are in Favor of ‘Privacy-Encroaching Technology’
Even as overall mortality data separating deaths “from” COVID and “with” COVID9 show COVID-19 is hardly the deadly pandemic it’s been made out to be, fear-mongering remains in full effect — including warnings on the more infectious, mutated strain of SARS-CoV-2, Delta. With fear still omnipresent, acceptance of “privacy-encroaching technology” that promises an illusion of safety is high.
In the U.K., researchers from the University of Bristol conducted two large surveys about such technologies, with overwhelming positivity reported.10 The first measured public acceptance of location tracking through your cellphone that would allow health agencies to monitor your contact with others to target social distancing and quarantine measures.
About 70% of the respondents said they would accept such an app that they could choose to download and, surprisingly, 65% also said they would accept such an app even if it was mandated by the government and used to locate those violating lockdown orders and issue fines and arrests.11
A second survey evaluated acceptance of vaccine passports, with 60% stating they were in favor and only 20% stating they were strongly opposed. The study’s lead author, professor Stephan Lewandowsky, described those opposed as “surprisingly low,” adding, “It’s fascinating how people seem increasingly receptive to their personal data being used to inform themselves and others about what they can and can’t do.”12
Prendergast put this widespread acceptance into further context for the British, who “have traditionally been deeply suspicious of the idea of an official asking for ‘papers, please’:”13
“[This] … is why there was such a backlash against Blair’s ID cards. As one journalist at the time put it:
‘If I am ever asked to produce my ID card as evidence that I am who I say I am, when I have done nothing wrong and when I am simply ambling along and breathing God’s fresh air like any other freeborn Englishman, then I will take that card out of my wallet and physically eat it in the presence of whatever emanation of the state has demanded that I produce it.’
That journalist is now our Prime Minister. It would be an extraordinary turn of events if Boris Johnson ended up being the man who introduced an immunity identity system in Britain.”
US Universities Institute Jail-Like Restrictions
At every turn, long-standing societal norms — like college students gathering with friends in their dorm or even leaving their rooms for work and exercise — are disappearing. As of February 7, 2021, for instance, the University of Massachusetts Amherst was in a “high risk” operational mode due to a “continuing surge in COVID-19 cases.”14
The status, which was to be in place for a minimum of 14 days, made all classes remote and ordered all students, whether residing on or off campus, to self-sequester in their residences, except to get meals, attend medical appointments or undergo twice-weekly COVID testing.
Violating these orders would result in “disciplinary action,” according to a university press release, which could include removal from residence halls or suspension.15 Students were also informed that, should they decide to leave campus to self-sequester at home, “it is highly unlikely we will be able to accommodate your return.”
Even within a residence hall, students were told to remain in their rooms at all times except when using a restroom on their floor. Outdoor exercise or attending to the immediate needs of a pet was allowed, but only when wearing a mask and maintaining social distancing.16
This wasn’t the case at UC Berkeley, however, which banned outdoor exercise in addition to extending dormitory lockdowns in February 2021. The only times students were allowed to leave their rooms during the lockdown were to obtain medical care, get required COVID tests, use an assigned bathroom or to obtain food from an outdoor dining kiosk, after which they were required to return immediately to their rooms.17
Are You Clean Enough to Travel?
While many countries have suggested that the COVID-19 vaccine will not be mandated, by giving special privileges to the vaccinated, such as the ability to travel, attend social events or even enter a workplace, it essentially amounts to the same thing and insinuates a “cleaner” class of people in those who have been vaccinated.
It’s reminiscent of the early days of the pandemic, when hand sanitizer and disinfectant wipes were flying off store shelves in a frenzy to clean away COVID. Now we know that transmission of COVID-19 by fomites — the term used for inanimate surfaces and objects that can transmit a pathogen — has been exaggerated.
Emanuel Goldman, a microbiology professor at Rutgers New Jersey Medical School, suggested this in July 2020, when he stated that studies suggesting SARS-CoV-2 was easily spread via surfaces did not present real-life situation.18
“In my opinion, the chance of transmission through inanimate surfaces is very small,” he said, and while period disinfection of surfaces, especially in hospitals, was a reasonable precaution, in public settings, he noted, “this can go to extremes not justified by the data.”19 In February 2021, an editorial in Nature supported Goldman’s work, suggesting that costly and toxic disinfection efforts are misguided.
“Catching the coronavirus from surfaces is rare. The World Health Organization and national public health agencies need to clarify their advice,” the editorial reads.20 Yet, the New York City Metropolitan Transit Authority alone is spending an estimated $380 million annually on COVID-related sanitation, and when it asked the U.S. government whether they should be focusing on fomites or solely aerosols, they were told to continue their focus on fomites.21
Writing in The Atlantic, Derek Thompson describes this as a type of “hygiene theater,” in which Americans are going through the motions of dutifully cleaning and, likely, over-disinfecting surfaces when the virus spreads most efficiently through the air.22
Indeed, much of the COVID-19 pandemic response has been embroiled in theatrics, including mask mandates, for which the scientific evidence has been described as “astonishingly weak.”23 Hygiene theater, much like the theater for vaccine passports, provides an illusion of safety, not one grounded in reality.
Discussion to Ban Florida Travel for Disobedience
In the U.S., Florida announced in December 2020 that it would have no more lockdowns and no statewide mask mandates.24 The act resulted in retaliation by federal government, which entertained the idea of a domestic travel ban to the state, reportedly to curb the spread of new COVID-19 variants.
In a press conference, Florida Gov. Ron DeSantis stated, “Any attempt to restrict by the federal government would be an attack on our state done purely for political purposes.” Florida’s U.S. Sen. Marco Rubio agreed, calling the act unconstitutional: “So now that they’re considering actual restrictions on Americans inside the country, I think it is unconstitutional. I think it’s going to be challenged in court successfully.”25
The “technocratic fascist vision”26 of professor Klaus Schwab, founder and executive chairman of the World Economic Forum who wrote the book on the Fourth Industrial Revolution, is moving ahead full-steam. He announced the World Economic Forum’s Great Reset Initiative27 in June 2020, which includes stripping all people of their privately-owned assets.
Getting health passports to become a new normal has, in fact, been part of the plan all along for the Commons Project, which began developing software that tracks medical data well before the COVID-19 pandemic. “But spikes in virus cases around the world this spring accelerated its work,” The New York Times reported.28
In the meantime, a widely-used medical records software called Epic is now capable of embedding your vaccination status29 into shareable charts from online patient portals such as MyChart. In turn, Epic has partnered with the Vaccine Credential Initiative,30 a coalition whose mission is to “provide digital access to COVID-19 vaccination records.”
Other partners with the Initiative are Mayo Clinic and Microsoft, with Microsoft creating the standards by which patients and designated others can get the vaccine and access records of it, as well as lab reports.
Coupled with the vaccine passports, which are starting out with the COVID-19 vaccine for international travel, it’s setting a precedent for expansion that can be extended to other vaccines and medical information, and then to domestic travel and even leaving your house, as the passports will be carried on your phone, which has location-tracking abilities.
And it’s clear that when the fascists come, they’ll be wearing masks — probably two or three of them31 depending on their level of loyalty. For now, getting informed and sharing your knowledge is the first step to protecting your freedom.
13 He that answereth a matter before he heareth it, it is folly and shame unto him. ~ Proverbs 18:13 KJV
Caught on Tape: J&J Officials Warn About COVID Shots
In this COVID vaccine investigative report, Johnson & Johnson scientists and journalists are secretly taped as they spill the beans on what they really think about their company’s vaccine. Their chilling and calloused remarks about the mass vaccination campaign will make your blood boil.
____________________________
People Injured by COVID-19 Jab Share Their Horror Stories
In June 2021, Wisconsin Sen. Ron Johnson held a news conference with families who shared stories about the injuries they’d suffered as a result of taking the COVID jab
September 10, 2021, WXYZ-TV Channel 7 posted a request on Facebook, asking people who had lost an unvaccinated loved one to COVID-19 to contact them for a story. The post has received more than 241,000 comments and most are about someone who was injured or died from the COVID shot, or who got severe COVID-19 despite being fully vaccinated
Jodi O’Malley, a registered nurse who works for the U.S. Department of Health and Human Services, is blowing the whistle on COVID jab injuries. Suspected vaccine injuries are not being reported, even though it’s required. In fact, few health care workers are familiar with this requirement and they don’t know how and where to file such reports
Brandon Schadt, a Johnson & Johnson regional business lead, has been caught on tape saying children should not get the COVID jab, and media cannot be trusted to tell the truth about the shots
Justin Durrant, a Johnson & Johnson scientist, agrees babies and young children don’t need the COVID shot, and tells the undercover reporter to not get the Johnson & Johnson COVID “vaccine”
At the end of June 2021, Wisconsin Sen. Ron Johnson held a news conference with families who shared stories about the injuries they’d suffered as a result of taking the COVID jab. You can watch the hour-long meeting, which was widely censored and suppressed, above.
While Johnson is diplomatic, stating that most people have no problem after taking the jab, and that the shots have saved many lives, it seems clear that side effects from the COVID injections are FAR more common than anyone is willing to publicly admit.
Case in point: September 10, 2021, WXYZ-TV Channel 7 posted a request on Facebook,1,2 asking people who had lost an unvaccinated loved one to COVID-19 to contact them for a story.
As of September 29, 2021, the post had more than 244,000 comments, and the vast majority are about someone who was injured or died from the COVID shot, or who got severe COVID-19 despite being fully vaccinated. You can browse through the hundreds of thousands of comments here. Below are some examples of the comments posted on the site:
“My good friend’s grandpa just passed away due to receiving his booster vaccine.”
“How about doing a story about my uncle who was in fine shape until he got vaccinated. Or my boss’s uncle who was healthy and in his 50s, then died suddenly a week after getting vaccinated.”
“My sister-in-law’s father died of a stroke 48H after Moderna vax. He was active and healthy.”
“What about my husband’s boss who had two strokes after her second dose?! Not interested in that story?”
“The shot murdered my friend three weeks after he got it.”
“I have a close friend that now has myocarditis after the shots. High Mortality within 5 years. Perfectly healthy prior to the shots.”
“I know 2 women who had strokes right after their shot.”
“We lost an uncle to heart inflammation 2 days after he received the vaccine.”
“Lost a very dear man after his second dose of the vaccine and he said he regretted getting it and he advised me not to get it. How about reporting on those? He died of a brain aneurysm, and was a very healthy man.”
“My beautiful mother passed away recently, 23 days after having the first AstraZeneca shot (that I didn’t know she was getting). ‘Immunization’ was the ‘cause of death’ on her death certificate.”
“I now know more people injured by the vaccine than people who even had covid.”
“No but I know of two people who died from Covid after being fully vaccinated.”
“My uncle passed away 3 months after his second shot. He was diagnosed with stage 4 colon cancer, had surgery, was released to rehab and then died of a blood clot. Thanks Pfizer.”
“I know two women who had miscarriages within 2 days of taking it.”
These responses are what you would call a major CLUE. As noted by one commenter, “Doesn’t sound like you’re getting the story you need judging by the vast majority of these comments about vaccine losses and side effects. Since there is such an overwhelming outpouring of vaccine reactions maybe do a story on that? There’s lots of people here to pool from it seems.”
We now also have medical insiders blowing the whistle, confirming COVID jab injuries are incredibly commonplace, and most are never reported. In an upcoming article, I will share businessman Steve Kirsch’s analysis that strongly suggests the reports in the U.S. Vaccine Adverse Events Reporting System (VAERS) is underreported by a factor of 41. This means there may actually be more than 200,000 deaths and up to 5 million COVID jab injuries.
HHS Whistleblower: ‘Evil at the Highest Level’
WARNING: PROFANITY
In a stunning Project Veritas report, Jodi O’Malley, a nurse working for the U.S. Department of Health and Human Services, reveals health officials are ignoring and covering up COVID-19 vaccine injuries.
O’Malley says she’s seen “dozens of people come in with adverse reactions,” including myocarditis, congestive heart failure and deaths, yet the reactions are not being reported. This, despite the fact that both the U.S. Food and Drug Administration and the U.S. Centers for Disease Control and Prevention require any suspected injury from an emergency use vaccine to be reported.
“If everyone is supposed to gather this data and report it, but no one is reporting it, how will anyone know the vaccine is truly safe? They don’t,” O’Malley says.
One of the reasons O’Malley decided to come forward, knowing she will likely lose her job over it, is because one of her coworkers who was coerced into taking the shot died. “Nobody should have to decide between their livelihood or take the vaccine,” O’Malley says.
She also points out that while there are medications such as ivermectin and hydroxychloroquine that have been shown to be safe and effective against the virus, the HHS will terminate anyone who uses these drugs. Were these drugs permitted, the COVID jab wouldn’t even qualify for emergency use. When O’Malley asks Gayle Lundberg, a DHHS pharmacist, if ivermectin can be given to a patient if the doctor is willing to prescribe it, Lundberg responds:
“I am stuck. I am told you are absolutely not to use [ivermectin] under any circumstances whatsoever for somebody with COVID, unless you don’t want to have a job. I’m not going to lose my job over this.”
“This is evil at the highest level,” O’Malley says. “You have the FDA, the CDC, that are both supposed to be protecting us, but they are under the government, and everything we’ve done so far is unscientific.”
Another whistleblower, Deborah Conrad, was recently featured in a Highwire exclusive. Conrad, a physician’s assistant, reveals there’s a complete disregard for the requirement to report COVID jab injuries at her hospital too. I will publish that interview this coming Friday, October 8, 2021.
Johnson & Johnson Officials Caught on Tape
WARNING: PROFANITY
In Part 3 of its COVID vaccine investigative series, Project Veritas exposes the true sentiments of two Johnson & Johnson officials: Brandon Schadt, a Johnson & Johnson regional business lead, and Justin Durrant, a Johnson & Johnson scientist.
Speaking to an undercover Project Veritas reporter over a meal, Schadt admits he does not agree with the push to vaccinate children. “Kids shouldn’t get a f*cking [COVID] vaccine,” he says. “It’s terrible … It’s a kid, you just don’t do that, you know? Not something that’s so unknown in terms of repercussions down the road.”
When asked if we really have no idea what the long-term repercussions are, he replies, “I mean, how could you? Right? There’s nobody who’s 30 years in who said, ‘Hey, I had the vaccine and I don’t have a third eyeball.” When asked if we can trust the media when it comes to reporting on the COVID shots, Schadt states, “In no capacity should we ever trust anything that they say.”
Durrant also doesn’t think babies and young children need the jab, saying “It wouldn’t make that much of a difference” if children are unvaccinated for COVID. That said, he does seem to be onboard with the corporate policy to push the injection on adults, regardless of need or personal beliefs.
He admits that what they’re doing is making life so inconvenient for the unvaccinated that they just give up and get it. Despite that, Durrant tells the undercover reporter: “Don’t get the Johnson & Johnson [COVID vaccine]. I didn’t tell you [that] though.”
FDA Warnings Issued for Janssen, Pfizer and Moderna
In late April 2021, the U.S. Food and Drug Administration added a warning label to the Janssen COVID shot about the risk for potentially serious blood clotting in the brain and other sites, including the abdomen and legs, in combination with thrombocytopenia (low platelet count), particularly among women.3,4 In mid-July, Guillain-Barre syndrome and altered immunocompetence were added to the list of warnings.5,6
In June 2021, Pfizer and Moderna both got warning labels added to their COVID shots as the FDA concluded there’s a “likely association” between the mRNA injections and heart inflammation in adolescents and young adults.7
June 24, 2021, Fierce Pharma reported that “heart inflammation has occurred at a rate of 12.6 per million among those aged 12 to 39, according to the CDC’s Vaccine Safety Datalink.”8
Menstrual Problems Emerging as a Widespread Side Effect
One of the side effects that has yet to register on the FDA’s and CDC’s radar is menstrual irregularities among women. According to a September 16, 2021, editorial in The BMJ,9 more than 30,000 reports of menstrual irregularities and vaginal bleeding had been filed with the British Medicines and Healthcare Products Regulatory Agency’s (MHRA) Yellow Card Scheme, which collects and monitors adverse vaccine reactions, as of September 2, 2021.
The editorial was written by Victoria Male, a reproductive immunology specialist at the Imperial College of London. According to Male, the link between these bleeding irregularities and the COVID jabs, irrespective of brand, is a plausible one that warrants further investigation. She writes:10
“Menstrual changes have been reported after both mRNA and adenovirus vectored covid-19 vaccines, suggesting that, if there is a connection, it is likely to be a result of the immune response to vaccination rather than a specific vaccine component.
Vaccination against human papillomavirus (HPV) has also been associated with menstrual changes. Indeed, the menstrual cycle can be affected by immune activation in response to various stimuli, including viral infection: in one study of menstruating women, around a quarter of those infected with SARS-CoV-2 experienced menstrual disruption.
Biologically plausible mechanisms linking immune stimulation with menstrual changes include immunological influences on the hormones driving the menstrual cycle or effects mediated by immune cells in the lining of the uterus, which are involved in the cyclical build-up and breakdown of this tissue.”
Assistant professor at University of Illinois at Urbana-Champaign, Dr. Kathryn Clancy, who is researching acute immune activation and menstrual repair mechanisms, told The Defender she’s “dismayed that the research design of [COVID] vaccine trials makes it impossible at this time to actually explore this relationship, and hope drug and vaccine manufacturers in the future take these considerations into account.”11
US Reports of Menstrual Irregularities
In the U.S., the Vaccine Adverse Event Reporting System (VAERS) had logged a total of 9,589 reports of menstrual disorders following a COVID injection as of September 17, 2021.12 Dr. Lawrence Palevsky, a pediatrician, also weighed in on The BMJ article, telling The Defender:13
“If we were to follow the scientific method, as it was taught in textbooks (knowing full well there is no longer any adherence to the scientific method), we would immediately see this observation of menstrual cycle changes in tens of thousands of women as a signal, for which necessary questions would need to be asked …
A true adherence to the scientific method would allow for answers to be reported without bias or prejudice for a desired outcome of the results … There is a long list of side effects that the manufacturers of the injection sent to the FDA in the fall of 2020.
Many of the injuries people are reporting after receiving these injections, including bleeding, blood clots, autoimmunity, Guillain-Barré syndrome and many others, are well known to the manufacturers and the FDA but, the powers that be continue to ignore the reports of people presenting with these real-time adverse events, as if they have nothing to do with the injections, at all.
Essentially, they gathered the data in clinical trials but have kept them completely under wraps.”
Palevsky believes the menstrual irregularities reported by women who have gotten the COVID shot may be related to effects from the spike protein that their bodies are now producing.
NIH Funds Study to Investigate Menstrual Irregularities
In early September 2021, the Institute of Child Health and Human Development and the Office of Research on Women’s Health, both of which are part of the National Institutes of Health, announced they will award $1.67 million in grants to five research institutions to investigate the link between menstrual irregularities and the COVID jabs.14,15
Over the next year, researchers at Boston University, Harvard Medical School, Johns Hopkins University, Michigan State University and Oregon Health and Science University, will try to determine whether the menstrual changes are directly linked to the COVID shots, how long the changes last, and what the underlying mechanism is.
The five studies are expected to enroll somewhere between 400,000 and 500,000 participants, according to Dr. Diana Bianchi, director of the Institute of Child Health and Human Development.
There’s also an independent group that is collecting data from unvaccinated women who are experiencing abnormal bleeding patterns after coming into close contact with a COVID jabbed individual. Palevsky and Dr. Christiane Northrup are part of this research group, among others. You can find more information about this project on MyCycleStory.com.16
In closing, while authorities insist the COVID shots are “safe and effective,” mounting data tell a different story. Not only are the injections losing effectiveness within months, as demonstrated by Israeli data discussed in the video above, VAERS has also received more than 726,960 adverse events reports following the COVID shot, including 15,386 deaths and 66,642 hospitalizations, as of September 17, 2021.17
These numbers are so staggering, there’s really nothing that can compare. In nine months, these shots have caused more VAERS reports of injury and death in the United States than all available vaccines over the past 30 years. A similar situation can be seen in the U.K., where 30,305 people have died within 21 days of their COVID shot. And that was just within the first six months of the vaccine rollout.18
In August 2021, Japan’s health ministry suspended the use of 1.63 million doses of Moderna’s injection after finding foreign substances that looked like metal particles in some vials. Then, in mid-September, suspected contaminants were discovered in a particular lot of Pfizer’s injection as well.19 Still, we’re told to just roll up our sleeves and ask no questions. Why?
As noted by Schadt, the Johnson & Johnson employee caught on tape by Project Veritas, the mass vaccination campaign isn’t really about public health, it’s about politics and money. Beyond that, I believe it’s about building the control mechanism needed for the Great Reset. Vaccine passports will allow unelected technocrats to control and manipulate the whole world according to their own whims.
As expected, it doesn’t end with two doses. In Israel, a fourth Pfizer shot is already being rolled out, and the year isn’t even over yet. And all those who took the first two doses will now lose all of their freedoms all over again, until they catch up on the recommended boosters. This is precisely what we can expect to happen everywhere else in the world, where vaccine passports are rolled out.
Freedoms are being tied to being up-to-date on your vaccinations, and once COVID-19 disappears, if ever, they’ll just come out with something else that must be injected into you if you want to work, go to school, travel, shop or live a semi-normal life.
This is what the new biosecurity state is built around. The question is, is that any kind of life? Is that how we want to live? Is this the world we want for our children and grandchildren? If not, we must all do our part and resist mandates, vaccine passports and restrictions based on vaccine status. The good news is, together we can win, because there are far more of us than there are of them.
13 He that answereth a matter before he heareth it, it is folly and shame unto him. ~ Proverbs 18:13 KJV
Here is a video by Pastor Keith Malcomson from Limerick City Church in Ireland that was uploaded by SermonIndex.net.
This is the sermon’s main biblical text,
14 And deceiveth them that dwell on the earth by the means of those miracles which he had power to do in the sight of the beast; saying to them that dwell on the earth, that they should make an image to the beast, which had the wound by a sword, and did live.
15 And he had power to give life unto the image of the beast, that the image of the beast should both speak, and cause that as many as would not worship the image of the beast should be killed.
16 And he causeth all, both small and great, rich and poor, free and bond, to receive a mark in their right hand, or in their foreheads:
17 And that no man might buy or sell, save he that had the mark, or the name of the beast, or the number of his name.
18 Here is wisdom. Let him that hath understanding count the number of the beast: for it is the number of a man; and his number is Six hundred threescore and six. ~ Revelation 13:14-18 KJV
Transhumanism is a technocratic system that is being pressed by the global elitists and especially by Klaus Schwab, founder of the World Economic Form (WEF) and driver of the Fourth Industrial Revolution that is bringing about the WEF’s planned and orchestrated Great Reset a.k.a. the New World Order. The COVID-19 pandemic is a planned global medical crisis that is being used as the scapegoat to bring about the Great Reset. Schwab, Prince Charles and many other global elitists have vociferously come out and said that the “COVID-19 pandemic has created an opportunity to reset the global economy.”1,2 The global coronavirus pandemic is nothing new as the world has experienced coronaviruses before. The National Library of Medicine states: “This is the third serious Coronavirus outbreak in less than 20 years, following SARS in 2002-2003 and MERS in 2012. While human strains of Coronavirus are associated with about 15% of cases of the common cold, the SARS-CoV-2 may present with varying degrees of severity, from flu-like symptoms to death.”3 The SARS (severe acute respiratory syndrome) CoV-1 and CoV-2 coronaviruses have flu-like symptoms that have been found to have a 99.998% chance of recovery and though deaths are reported to occur, so do deaths occur with the influenza.4 This pandemic found its roots also more recently in Event201 which you can also read extensively about at The Coronavirus Plandemic blog of 28th October 2020, where I wrote:
Preceding the “outbreak” of the coronavirus epidemic which quickly spread around the world and became known as a pandemic, a so-called fictitious exercise was undertaken by The Johns Hopkins Center for Health Security in partnership with the World Economic Forum and the Bill and Melinda Gates Foundation. The Event201, described at the website as “a high-level pandemic exercise”, was hosted on 18th October, 2019 in New York, NY. The Event201 description at the The Johns Hopkins Center for Health Security website reads: “A GLOBAL PANDEMIC EXERCISE”.
This is the demonic work of antichrists who are messing with the Creator GOD’s divine order and knowingly or unknowingly they are fulfilling GOD’s Word in this very present age. In scripture we read about the fall of Babylon from a historicist context, yet we find ourselves in a parallel age that is a repeating of history. We read of sorceries that are present which deceived all nations – is that not what we see today? For we read,
23 And the light of a candle shall shine no more at all in thee; and the voice of the bridegroom and of the bride shall be heard no more at all in thee: for thy merchants were the great men of the earth; for by thy sorceries were all nations deceived.
24 And in her was found the blood of prophets, and of saints, and of all that were slain upon the earth. ~ Revelation 18:23,24 KJV
The word “sorceries” in this text is the Greek word pharmakeia (φαρμακεία) from where we get the English words ‘pharmacy’ or ‘pharmaceutical’. Strong’s Concordance #5331 reads as follows: φαρμακεία pharmakeia far-mak-i’-ah From G5332; medication (“pharmacy”), that is, (by extension) magic (literal or figurative): – sorcery, witchcraft.
This is what we are experiencing right now in the world that nations are being deceived with the sorceries of the big pharmaceutical companies as governments are coercing and forcing the gene therapy jabs of the FDA’s emergency authorised use (EAU) “vaccines” manufactured by Pfizer, Moderna, Johnson & Johnson, Oxford-Astrazenica, et al upon the global population. These vaccines are causing adverse effects/injuries and even death, yet the governments push the vaccination narrative to get as many people vaccinated as possible. The end result will be that people will eventually give in to carry vaccination passports that will cause a medical apartheid where those who received the jab will have first rate benefits and freedoms and the second rate un-vaxxed people will not. It will bring about the new capitalism that is global socialism controlled by the mega rich elitists who will control everything. This is how the Great Reset will function.5 These are just the precursor days that will lead towards “… And that no man might buy or sell, save he that had the mark, or the name of the beast, or the number of his name. Here is wisdom. Let him that hath understanding count the number of the beast: for it is the number of a man; and his number is Six hundred threescore and six.” (Revelation 13:17,18 KJV). The vaccination passports that the governments are pushing for will prohibit entering into certain establishments, restaurants, sports stadia, travelling on aeroplanes, and the like. Only time will tell and come to pass.







")












 The European website can be viewed at
The European website can be viewed at 




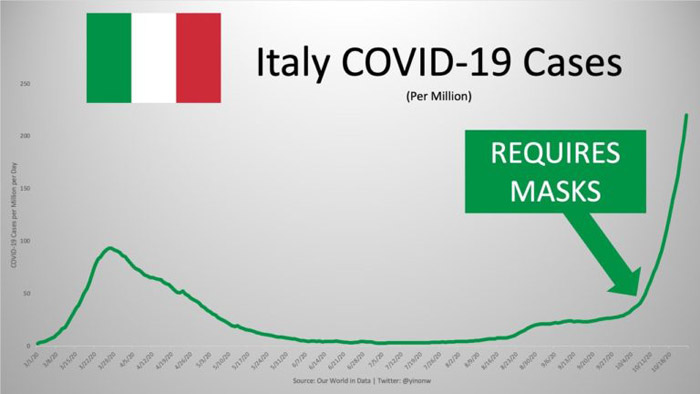
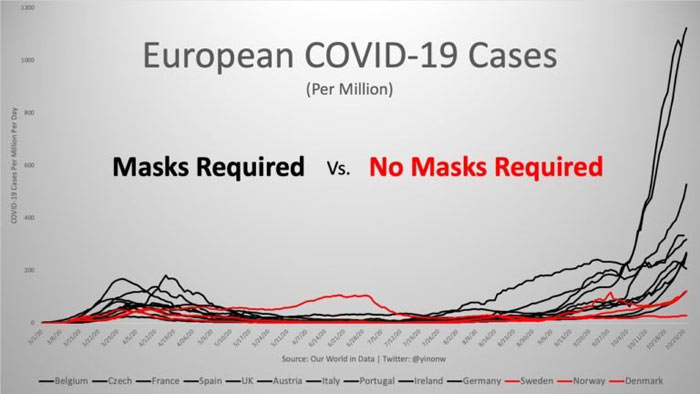

 STORY AT-A-GLANCE
STORY AT-A-GLANCE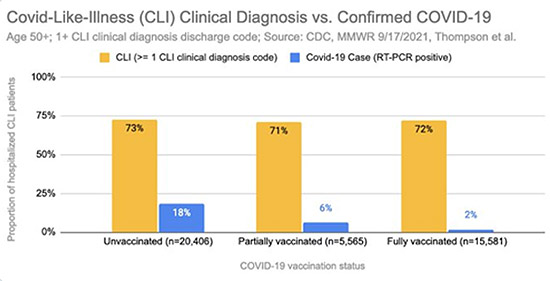



 STORY AT-A-GLANCE
STORY AT-A-GLANCE


 Joshua Project
Joshua Project The Biblical Basis of Missions
The Biblical Basis of Missions

![The Nativity of our Lord Jesus Christ ~ Luke 1 & 2 The Biblical Nativity (Birth) of our Lord Jesus Christ according to the Holy Scriptures in the Gospel of Luke 1 & 2 [see Purge the leaven … blog post]](https://luke923evangelism.files.wordpress.com/2012/12/birth-of-christ.png "The Biblical Nativity (Birth) of our Lord Jesus Christ according to the Holy Scriptures in the Gospel of Luke 1 & 2 [see Purge the leaven … blog post]")